Studying drug safety in pregnancy: The contribution of the PROTECT project

The safety of medicines during pregnancy remains one of the most complex and least explored areas of medicine. Pregnant women are generally excluded from clinical studies, and animal models do not always manage to predict accurately the effects of drugs on the human foetus.
To fill this gap, PROTECT was created, a project that won an ERC Proof of Concept grant, led by Professor Alessandro Filippo Maria Pellegata within LaBS-3DBioprinTE – Laboratory of 3D Bioprinting and Soft Tissue Mechanics.
Why is drug safety in pregnancy still an area with so many scientific uncertainties today?
The main reason is that, during pregnancy, a principle of maximum caution applies: if the effects of something are not known with certainty, it is avoided as a precaution. This is because it is extremely difficult to conduct direct studies on the foetal toxicity of drugs. As a result, for many drugs it is not known precisely what the effect on the foetus is during pregnancy and, in order not to run risks, it is preferable not to administer them.
There have been striking cases in history of drugs initially considered safe that later proved harmful to the foetus. For this reason too, a particularly cautious approach is adopted today.
There are numerous studies on toxicity in the initial stages of pregnancy, particularly during embryonic development. Data relating to the later stages, such as the second and third trimester, are much more limited.
And why are there more studies on the embryonic stage than on the more advanced one?
Partly because there is already extensive scientific literature on the embryonic stage. This interest did not originally arise from the study of the foetal toxicity of drugs, but rather from developmental biology: the aim was to understand the mechanisms and processes that take place in the earliest stages of life. This has led to the availability of numerous experimental models for studying embryonic development.
Within your research project, are you focusing on specific trimesters or stages of pregnancy?
Yes. The cells we are able to obtain come from pregnancies of at least 17 weeks’ gestational age. This means that we work mainly on the second and third trimester. Earlier than that would in fact be much more complicated, at least not with minimally invasive and safe procedures. Any sampling must take place without introducing additional risks for the mother. This constraint inevitably limits the period we can work on.
What are the main risks for pregnant women when they need to take medicines?
The risks exist on two distinct but interconnected levels: the maternal and the foetal.
On the one hand, there is the risk that a drug may have toxic effects on the foetus, interfering with its development. On the other hand, however, failing to administer a drug can represent a problem for the mother’s health, especially in the presence of chronic or progressive conditions.
An emblematic example concerns some neurodegenerative diseases, which require continuous therapies to slow the progression of symptoms. In these cases, interrupting treatment can have significant consequences. There are situations in which a woman, at the moment she decides to have a child, has to stop treatment for a very long period: not only during pregnancy, but also in the months before conception — to allow the drug to be eliminated from the body — and during breastfeeding. This can result in an overall interruption of treatment lasting as long as two or three years, with potential repercussions for maternal health.
Alongside these more critical aspects, there is also a dimension linked to quality of life. Some medicines, not necessarily life-saving or linked to chronic therapies, which improve everyday wellbeing, are not used during pregnancy because of the uncertainty surrounding their effects.

What is your academic and professional background? What led you to become interested in this field?
My academic path took place mainly at Politecnico di Milano, where I graduated in Biomedical Engineering and then obtained a PhD in Bioengineering. During my PhD I began working in the field of regenerative medicine, dealing with the development of engineered solutions, based on biotechnological techniques, for the reconstruction of organs and tissues.
I then moved to London, where I worked for several years as a postdoctoral researcher at UCL. There too I worked in regenerative medicine, a field in which I still work today, with a particular focus on the paediatric context: both on congenital conditions, therefore diagnosable also during the prenatal stage, and more generally on conditions linked to the prenatal and neonatal period.
How did the idea for the PROTECT project come about?
The idea arose from the convergence of different elements. On the one hand, in recent years of research I developed strong expertise in the study of amniotic fluid cells. On the other, my interpersonal experiences also played a role, linked to people who found themselves facing difficulties in the management of drug therapies during pregnancy. Added to this was the experience gained in the field of in vitro modelling.
Bringing these three aspects together — technical skills, research experience and awareness of the clinical problem — the idea for the project emerged: to develop a tool that can help increase knowledge of the effects of drugs on the foetus during pregnancy.
What are the various phases of the project and which phase are you in at the moment?
The aim of the project is to develop an experimental platform in which cells from amniotic fluid are organised into three-dimensional structures through bioprinting techniques. In practice, this means “printing” small three-dimensional constructs containing these cells, in a standardised, repeatable and reproducible way on a large scale.
Once this system has been created, the next step will be validation of the model. Before being able to generate new knowledge, in fact, it is essential to demonstrate that the model is reliable and able to reproduce already known results. For this reason, in this first phase — which coincides with the duration of the project, equal to 18 months — we will test drugs whose foetal safety or toxicity profile is already known, on the basis of clinical data and retrospective studies. The objective is to verify that the in vitro model is able to reflect what happens in vivo.
Subsequently, in a more advanced phase that will require further funding, it will be possible to expand the system and use it to produce new knowledge.
As for the current status, we have already conducted preliminary studies that have allowed us to collect data and demonstrate the feasibility of the approach. We are already able, on a reduced scale, to create these three-dimensional constructs containing amniotic fluid cells.
During the project we will work to make the process increasingly standardised, controllable and scalable — essential characteristics for a reliable experimental model.
What exactly is meant by “experimental platform”?
In this context, it means an integrated system that includes several elements: the cells, a support material (such as a gel) into which the cells are inserted, and a set of controlled experimental conditions that allow them to grow and be tested in a repeatable way.
In practice, one can imagine a structure composed of many small compartments — the so-called “wells” — inside which these three-dimensional constructs are cultured. In each well it is possible to place cells from different patients and test different drugs at varying concentrations.
By scaling up this approach, it becomes possible to test many patients, numerous drugs and different concentrations at the same time, generating hundreds or thousands of experimental conditions in parallel.
Turning to the technical side, what does it mean to print foetal tissues with 3D bioprinting? How does it work?
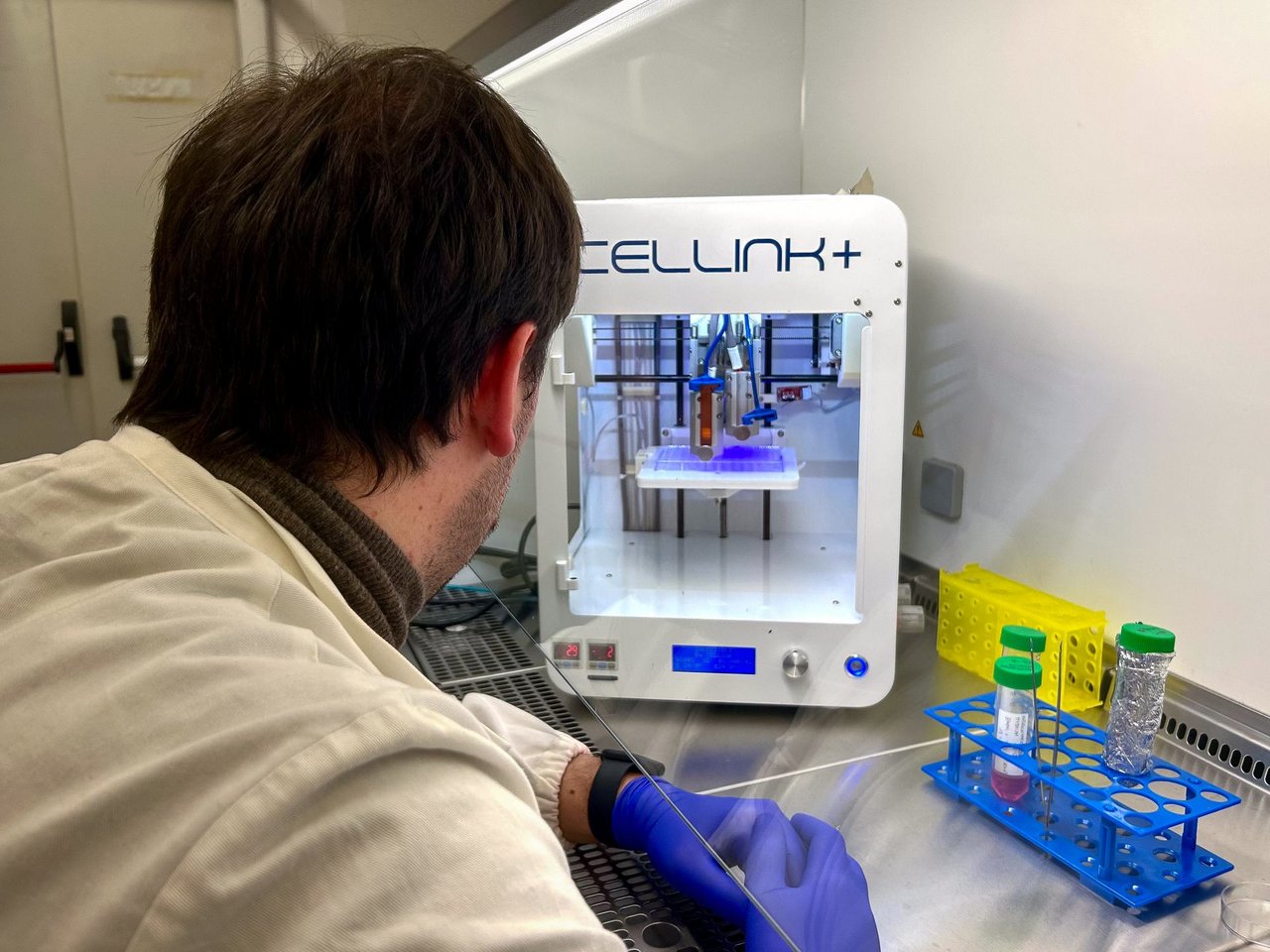
3D bioprinting is a technology based on principles similar to those of traditional printing or 3D printing: in particular, some techniques involve depositing a material, layer by layer, until a three-dimensional structure is formed.
In the case of bioprinting, however, instead of plastic materials or inks, biomaterials are used — generally gels with suitable biological properties — that contain living cells within them. In this way, real three-dimensional biological constructs can be “printed”, composed of a supporting matrix and cells.
Why are cells derived from amniotic fluid particularly suitable for creating these models?
There are two main reasons. The first is that these cells make it possible to build in vitro models that directly reflect the biological characteristics of the foetus.
The second concerns accessibility: this is in fact a cellular source that can be obtained without excessively invasive procedures and without particular ethical concerns. In many cases, amniotic fluid is already collected as part of clinical procedures such as amniocentesis or other prenatal interventions, for example for diagnostic purposes.
Who makes up your research group and who do you collaborate with?
Ours is a strongly multidisciplinary group, precisely because we work on very different and cross-cutting themes. Within it there is expertise ranging from biomaterials to bioprinting, from cell biology to bioinformatics, all the way to the clinical field: we collaborate in fact with paediatric surgeons and gynaecologists. This variety reflects the complexity of the research questions we address.
On the scientific level, we collaborate with some leading international centres: Bambino Gesù Hospital in Rome, the hospital and the university of Leuven in Belgium, and UCL in London. These are institutions that are very active in the fields of foetal surgery, regenerative medicine and prenatal and neonatal research. Collaborations with these centres are not limited to this project, but are part of a broader and well-established working network.
What could be the medical and social impact of the project?
The main objective is to develop a tool that is currently lacking: a reliable system for evaluating the effects of drugs on the foetus. If this tool proves valid, it could in future be used to test new drugs. In this sense, the immediate impact of the project is methodological: to create a solid basis on which to build subsequent studies.
Looking ahead, a model of this kind could also have broader implications. It fits, for example, into the context of personalised medicine, an approach that is increasingly central in biomedical research, especially in oncology. It is now clear that different patients can respond very differently to the same therapies, depending on genetic, environmental and individual factors.
What are the main challenges you are facing?
From a scientific point of view, the main difficulty concerns building in vitro models that are truly representative of biological reality. When a model is developed, in fact, many simplifications are inevitably introduced compared with the complexity of a living organism. The challenge lies precisely in understanding which simplifications are acceptable and which, instead, risk compromising the reliability of the model. Arriving at a system capable of convincingly reproducing what happens in the human being is, without doubt, the greatest obstacle.
What has struck you most, from both a scientific and a human point of view, while working on this project?
One of the most significant aspects, also on a personal level, concerns the way pregnancy is experienced. There is still, at least in part, a cultural view according to which pregnancy is treated almost as though it were a pathological condition, whereas in reality it is a physiological state. Today, fortunately, this view is changing: there is growing recognition that during pregnancy it is important to maintain, as far as possible, an active lifestyle.
In this sense, one of the aspects I care most about is that, in the long term, projects such as this may help improve the quality of life of pregnant women. The aim is to prevent pregnancy from being experienced as a period of renunciation — whether this concerns medicines that are useful for everyday wellbeing or, in more complex cases, therapies that are fundamental for the mother’s health.
In general, the idea is to contribute to a view of pregnancy that is increasingly close to its physiological nature.
You might also like

In the laser museum where physics tells its story
Period instruments and pioneering prototypes trace a century of research, all the way to ultrafast lasers and attosecond science.
Bobsleigh, bicycles, wheelchairs and feet: Lecco’s HexaLab is the world’s most advanced multi-sport simulator
The HexaLab at the Lecco Campus is based on the “human-in-the-loop” approach, whereby a human operator can control the simulator and physically interact with the equipment and the “simulated” environment around them

Art, science and technology in the unique design of Horacio Pagani’s hypercars
A close-up with the Italian-Argentinian entrepreneur, founder of Pagani Automobili, who revolutionised the automotive sector with his talent
